Case Notes:
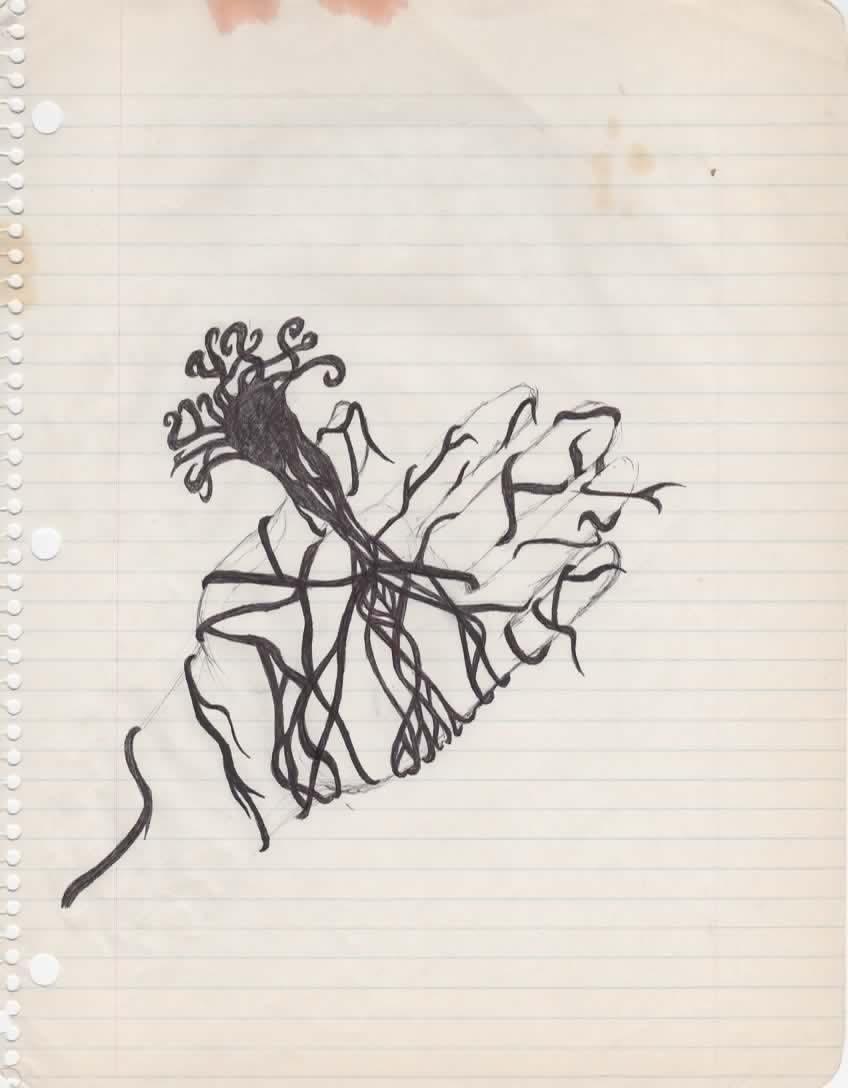
Client drawing: Tainted Hand
Medium: Black ink on lined notebook paper
0. Situating the Piece: A Plan More Than a Picture
I am reading Tainted Hand less as “a drawing of a hand with roots” and more as a Plan in the Deleuzian sense—an operational map for getting out of a situation of institutional stasis (classroom time) by carefully engineering a controlled deterritorialization.
The client reports this was done in class, in a bored state, but with very deliberate attention to proportion and line. The piece feels like an agreement the client made with themselves:
If I stay within a certain discipline (realistic hand, clean lines), I’m allowed to leave the classroom, conceptually, by letting the roots take over.
This is not the expression of a trauma story; it is a manual for how to escape a rigid temporal stratum without blowing the system up.
1. The Tainted Hand as Assemblage
Assemblage: Plan for Controlled Deterritorialization from Classroom Time
1.1. Session Notes: Initial Read on Operational Components
1.1.a. The Partial Object – “The Hand” The hand is proportionally accurate, contained, and technically assured. There is no mutilation, no severing: the transformation comes through the hand, not at the expense of it. Clinically, this reads as: the client needs a stable operator—a competent, useful organ—to serve as launchpad for any escape. No psychotic dissolution here; it’s a disciplined line of flight. The careful rendering suggests that the client’s capacity to sustain concentration under boredom is high. In other health and behavior-change contexts, “sufficient intensity” and sustained engagement are crucial preconditions for a successful intervention (Dennis et al., 2012). Here that “intervention” is self-directed: drawing becomes the client’s own intensive program for altering their affective state while remaining physically in class.
1.1.b. The Stratum – Lined Notebook Paper as Code of the Institution The lined paper is the pedagogic grid: horizontal rules, perforated margin, the language of “stay inside the lines,” “take notes,” “pay attention.” The perforated edge records a first molecular break: the page has already been torn out of its book—small but real separation from the school machine. In schizoanalytic terms, this is the school stratum: a stable arrangement of bodies, times, and expectations. The drawing is executed on this code rather than on neutral art paper, so the assemblage is inherently dialoguing with (and against) institutional time. There is an analogy here with how health systems embed patients within structured programs. Reviews of primary care interventions have noted that organizational structures can either support or constrain meaningful change depending on how flexibly they allow patients to engage (Dennis et al., 2012; Khatri et al., 2024). The notebook lines occupy a similar function for the student: a pre-written script of how time should be used.
1.1.c. The Speed Vector – Ink as Anti-Stasis Thick, unmodulated black ink: once the line starts, it commits. There’s no erasing; corrections are done by over-layering or accepting “errors” as part of the form. This density reads as a local intensification of time: the hand moves faster and more decisively than the classroom’s slow drip. From a process standpoint, the ink flow is the speed vector of the assemblage. It is how the client actively disrupts “flat” clock time in class and replaces it with an internal time of concentration and micro-decision. In other domains, we see how intensity and continuity of engagement are key—whether in lifestyle change interventions (Dennis et al., 2012) or community mental health programs that must maintain contact amid structural constraints (Khatri et al., 2024). Here, the ink is the client’s way of maintaining an inner continuity of experience in a setting they experience as deadening.
2. Molecular Invasion: Becoming-Root Rather Than Falling Apart
Once the hand is established as a competent partial object, a second phase begins: the molecular invasion. From the fingertips (and/or palm), black tendrils extend and proliferate, forming something between roots, veins, mycelia. I read this in the notes as becoming-root: the hand ceases to be only a social organ (“for writing, for raising in class”) and becomes an organ for anchoring, sensing, and spreading under the surface.
2.1. Positive OwB
OwB – Becoming Non-Human Without Loss Crucially, the hand is not severed. There is no dismemberment, no empty space where a limb should be. The figure is not about lack; it is about overgrowth. In clinical language: No clear indications of body-horror, castration anxiety, or self-directed violence. Instead, we see curiosity about what happens when an organ exceeds its assigned function. So, rather than a defensive fragmentation, this looks like a positive Body without Organs operation: a restructuring of use and relation without destroying the form. The hand keeps its shape but changes its job. With adolescents, this is especially significant. Post-COVID work on adolescent mental health has shown high rates of internalizing symptoms, but also a strong need for community-based, creative interventions that allow youth to experiment with identity and roles without being locked into a pathological label (Saha et al., 2022).
2.2. Contagion Vector V4
V4 – Rhizome as Affective Coupling The root system functions as a contagion vector: Every new line that branches off is a tiny wager: “I can still keep this coherent.” Each branch ignores the notebook’s lines, crossing them, sometimes echoing them, but never submitting fully. The feeling I read (and would check against the client’s own report) is not fear but a kind of low-key exhilaration: “I’m getting away with something on this page. It still looks like ‘a hand’ (so I’m safe), but it’s also not what the page is for (so I’m free).”
From a schizoanalytic standpoint, the anxiety of being a good student is gradually replaced by the pleasure of coupling—the sensation of hand + ink + root patterning as a living, evolving configuration. This is consistent with how some intervention frameworks emphasize shifting from compliance-based models to partnership and co-creation, where the person’s own experiential knowledge leads the process (Butenko et al., 2017; Dennis et al., 2012). The client isn’t passively filling in a worksheet; they’re generating a personal cartography of escape.
3. Stratum-Resistance: Ignoring the Lines as Final Break
The client notes that they ignored the notebook lines while drawing. This matters.
3.1. Overwriting the Pedagogic Code
Standard use: lines guide linear text, equal font size, uniform spacing. Actual use: the root-lines slice diagonally, curve, cross, and sometimes run parallel only incidentally. The earlier “function” of the page (note-taking, test answers) is repurposed into a planetary surface for root-growth. Clinically, I read this as a micro-political act: not dramatic enough to get the client in trouble, but sufficient to re-own the space of the page. The break with the code is not a tantrum but a quiet capture: the drawing uses the institutional support (paper, lines, class time) as fuel for its own agenda. There is a provocative analogy here with how clinical NLP systems “normalize” free text into controlled vocabularies (Henry et al., 2020). In a parallel way, a traditional clinical reading might try to normalize this drawing into one of a small set of interpretive categories.
3.2. Clinical Resistance – Refusing Concept Normalization
From an art-therapeutic perspective, I see a potential risk: that I, as therapist, become like a concept-normalization algorithm. I might be tempted to map terms onto existing diagnostic or symbolic lexicons. This parallels how keyword extraction systems (Khan et al., 2022) or clinical concept normalization tools (Henry et al., 2020) operate. But Tainted Hand is doing the opposite: it denormalizes the ruled page. It insists that the lines are just one material among others to be drawn over, not the master code. This stance resonates with broader movements in health research that stress the importance of honoring patients’ own lived experiences and metrics (Inceer & Mayo, 2024). In both cases, the question becomes: “What does this assemblage do for this person in this context?” rather than “To which category does this artifact belong?”
4. Working With the Plan Clinically
4.1. How I Might Speak With the Client About It
In session, I would likely keep my language grounded and concrete. The goal is to stay with the experience of becoming, not to drag it back into a pre-scripted narrative. This is akin to what community-based interventions for adolescent mental health are trying to do post-COVID (Saha et al., 2022).
4.2. Tracking the Affective-Archive
If this image reappears across time, it could start to function as part of the client’s Affective-Archive: A portable, repeatable way of slightly loosening institutional or relational constraints. A reminder that they can change the “job” of a body part without destroying it. I would be attentive to patterns of correlation (Saha et al., 2022), but my aim would be to keep the archive productive, not merely descriptive.
4.3. Contract of Interpretation
Implicit in all this is a contract: I will not pre-normalize your drawing into my codes. You are not obliged to give me a trauma story to justify its existence. We can follow what it does before we decide whether any of it needs to be “fixed.” This is similar in spirit to models of clinician–patient partnership (Butenko et al., 2017), where the patient’s willingness to participate depends on whether their role is respected. In art therapy, the drawing itself is one of the partners.
5. Provisional Clinical Formulation
Risk: Low evidence, in this image alone, of acute self-harm or psychosis.
Function of the image: Self-organized exit from institutional boredom. Experiment in reassigning function to a socially over-coded organ. Quiet reappropriation of institutional material as space of personal freedom.
Schizoanalytic stance: Treat Tainted Hand as a Nomadic Machine, not a symptom. Track intensities and flows instead of hunting for latent meaning. Support the client’s capacity to design and refine such Plans without forcing them back into diagnostic normalization.
Further work would involve inviting new images that continue or interrupt this motif, then mapping how each iteration negotiates with different strata, always foregrounding the client’s own experience as primary data.
References
Butenko, S., Lockwood, C., & McArthur, A. (2017). Patient experiences of partnering with healthcare professionals for hand hygiene compliance: A systematic review. JBI Database of Systematic Reviews and Implementation Reports, 15(1), 1645–1670.
Dennis, S., Williams, A. M., Taggart, J. R., Newall, A. T., Denney-Wilson, E., Zwar, N., Shortus, T., & Harris, M. (2012). Which providers can bridge the health literacy gap in lifestyle risk factor modification education: A systematic review and narrative synthesis. BMC Family Practice, 13(1), 44.
Henry, S., Wang, Y., Shen, F., & Uzuner, Ö. (2020). The 2019 National Natural language processing (NLP) Clinical Challenges (n2c2)/Open Health NLP (OHNLP) shared task on clinical concept normalization for clinical records. Journal of the American Medical Informatics Association, 27(5), 721–729.
Inceer, M., & Mayo, N. E. (2024). Health-related quality of life measures provide information on the contributors, components, and consequences of frailty in HIV: A systematic mapping review. Quality of Life Research, 33(6), 1735–1751.
Khan, M. Q., Shahid, A., Uddin, M. I., Roman, M., Alharbi, A., Alosaimi, W., Almalki, J., & Alshahrani, S. M. (2022). Impact analysis of keyword extraction using contextual word embedding. PeerJ Computer Science, 8, e839.
Khatri, R., Endalamaw, A., Erku, D., Wolka, E., Nigatu, F., Zewdie, A., & Assefa, Y. (2024). Enablers and barriers of community health programs for improved equity and universal coverage of primary health care services: A scoping review. BMC Primary Care, 25(1), 22.
Saha, I., Majumder, J., Bagepally, B., Ray, S., Saha, A., & Chakrabarti, A. (2022). Burden of mental health disorders and synthesis of community-based mental health intervention measures among adolescents after the onset of COVID-19 pandemic time in low middle-income countries: Protocol for systematic review and meta-analysis. International Journal of Noncommunicable Diseases, 7(1), 46–51.
Comments
Post a Comment